Technologies originally designed for neurovascular procedures can also be utilized in non-neuro interventions. This lecture will discuss several related topics.
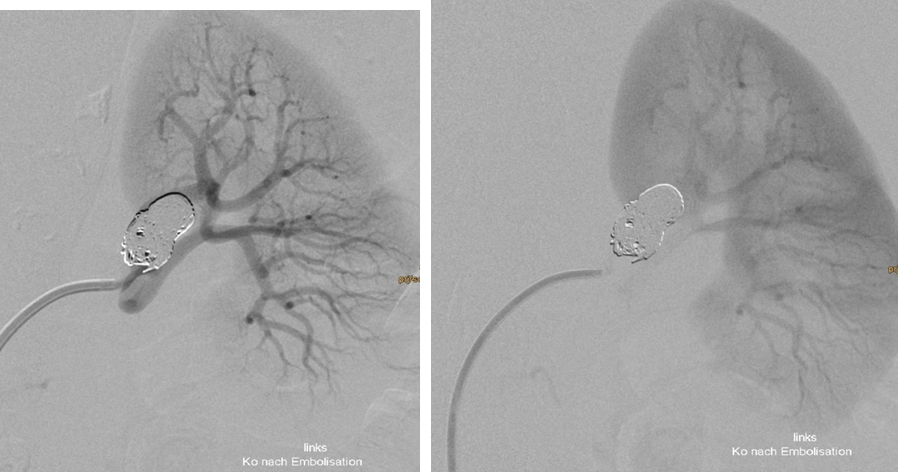
Treatment of complex aneurysms: Treatment of complex intracranial aneurysms often involves balloon-remodeling, stent-assisted coiling, or flow diverters. These methods can also be used for non-neurovascular procedures, specifically in treatment of visceral aneurysms. Renal artery aneurysms are most frequently located in the renal hilum, where the main renal artery diverts into its ventral and dorsal branch. Preservation of all renal artery branches may request advanced techniques as mentioned above (1); Fig 1,2.
Flow-induced aneurysms located at the pancreas arcade may also be quite complex in their angioarchitecture, quite often they are multiloculated and or fusiform. Stent-grafts intended for use in the coronary arteries typically lack suitability for these sites, as their diameter is often too small and their length is too short. Conversely, stent-grafts manufactured for peripheral applications tend to be too rigid and require larger introducer systems, which may not be appropriate for these locations. Therefore, the flow-diverter technology may be applied in these type of aneurysms. Recently, large diameter flow diverters with a diameter up to 8 mm have become available. An on-going multicentric study will evaluate these devices clinically (2,3).
Embolisation: Ethylene vinyl alcohol copolymer (EVOH) based embolization agents have been first used in treatment of cerebral arterio-venous malformations (AVM´s). The advantage of this type of embolization devices compared to alternatives is the non-adhesive character and the “lava-like” flow properties. This makes the application of the embolic material very controllable. After well documented benefit in brain AVMs EVOH based embolic angents have been used in several non-neurovascular embolization procedures like peripheral AVMS; embolization of endoleaks after EVAR procedures and also tumor embolization.
Thrombus removal: Although thromboaspiration from peripheral arteries has been introduced many years ago, the technique of transarterial aspiration thrombectomy in patients with acute ischemic stroke has strongly influenced non-neuro thrombectomy. Highly flexible large-bore aspiration catheters are now available also for peripheral arteries, which make peripheral thromboaspiration often much more effective than in former times (4). In selected cases, aspiration thrombectomy may be also combined with retriever thrombectomy, like it as applied in treatment of acute ischemic stroke.
This specifically accounts for mesenteric embolie, where highly flexible but still rather large aspiration catheters are required.
Influenced by the technology of cerebral aspiration catheters large bore catheters with an diameter up to 24F have been developed for pulmonary thrombectomy treatment in high risk and intermediate high risk patients with pulmonary embolism. Although large bore thrombectomy in pulmonary embolism is still under investigation, it may be assumed that this treatment concept will be a game-changer in the treatment of acute pulmonary embolie.
In summary, neurovascular techniques conceptually influenced non-neuro interventions in 2 ways: First the technique applied – second the development of devices.