Reduced recurrence rate
Appropriate patient selection is probably the most effective way to reduce treatment failure, by targeting sufficiently symptomatic patients and carefully excluding differential diagnoses such as tumours or anal fissures (6). The success rates reported in the literature are high, ranging from 63% to 94%, with no major complications (7).
Bleeding recurrence remains the main cause of clinical failure and occurs in our experience in one third of cases (4). It can be managed either with repeat embolization or by referral for proctological or surgical treatment.
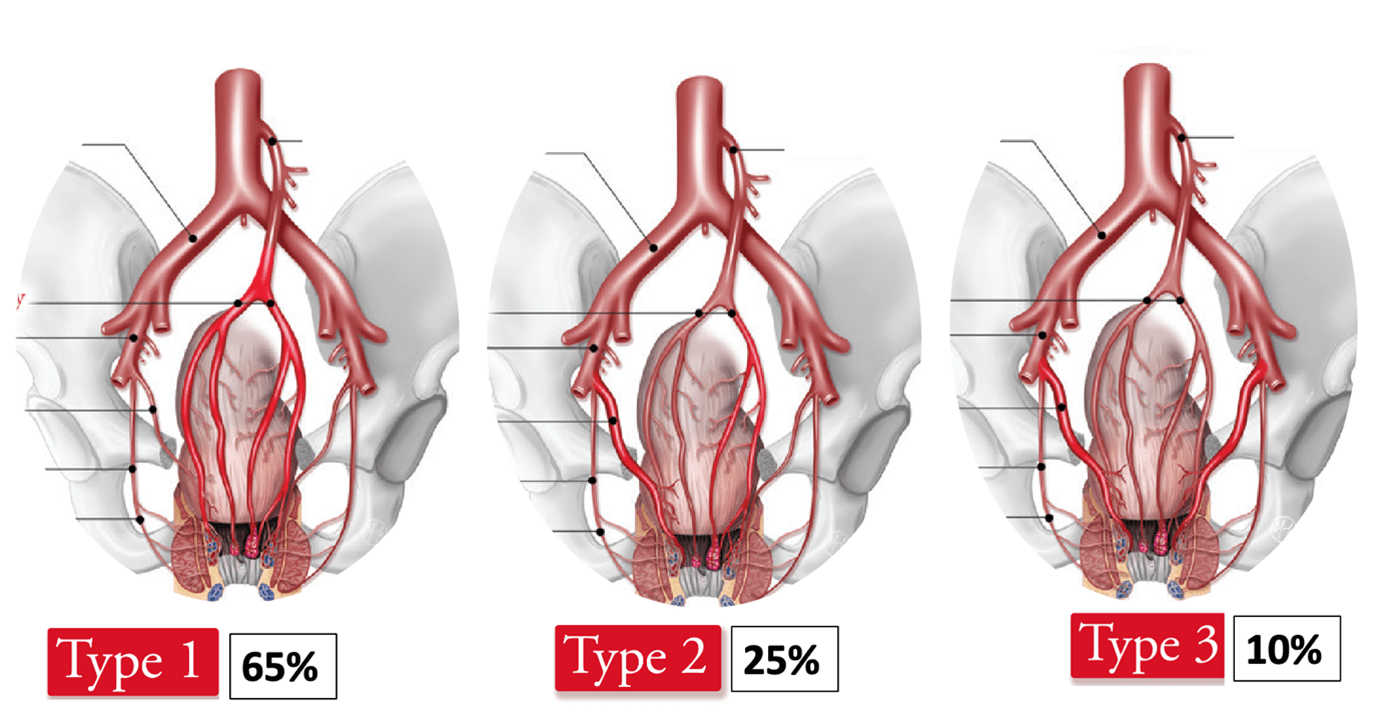
This raises the question of whether routine embolization of a hypertrophic middle rectal artery (MRA) should be performed during the initial procedure. When the MRA is of significant caliber, it appears reasonable to embolize it in addition to the SRA. Embolization of the MRA may help reduce the risk of symptom recurrence and the need for repeat embolization in the long term (8).
The use of cone-beam CT–based embolization planning software may facilitate identification, segmentation, and navigation of the MRA, particularly through augmented fluoroscopy guidance (5).
Embolic materials
The highest efficacy rates have been reported with the use of large microspheres combined with microcoils (9). Microspheres allow more distal embolization within the corpus cavernosum recti (CCR). However, the rate of minor complications is higher, approaching 50%, and mainly consists of small ischemic ulcerations of the anorectal junction (9). At present, there is insufficient evidence to recommend particle embolization over coil embolization (8). According to the available literature, large microspheres (>700 μm) delivered through selective and non-wedged infusion targeting a hypertrophied CCR, appear to be safe, and their use may reduce the recurrence rate compared with coil embolization alone.
Liquid embolic agents are not recommended for hemorrhoidal embolization because of the risk of anorectal ischemia (10).